












LYMEPOLICYWONK: CDC outreach to Lyme community—true patient engagement or tokenism?
The CDC has shown a willingness to talk to Lyme patient advocates lately. Is that a breakthrough, or not?
The CDC has made significant overtures to the community lately—meeting with patient groups, sharing information of breaking events and answering questions. One of the issues that the patient groups struggle with is determining whether these outreach efforts are genuine exercises in engagement that could provide patients with a meaningful voice in health policy matters that affect their lives (like treatment options) or whether patients are merely being placated .
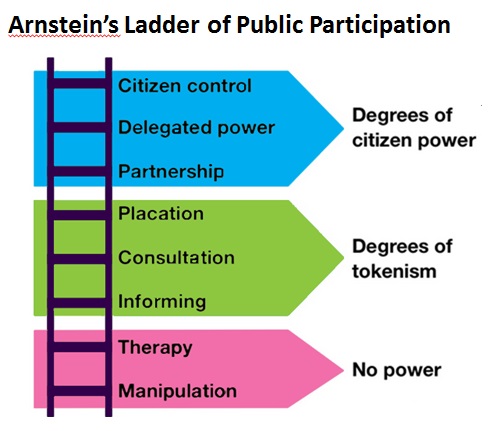
What is the difference between true engagement and tokenism? It’s a matter of whether patients have a real opportunity to influence decision-making or not. Sherry Arnstein is best known for laying out the different levels of citizen engagement in a democracy, which she illustrates with the so-called “Arnstein ladder.” The bottom rungs of the ladder provide no real opportunity for citizen influence and are regarded as either a form of manipulation or tokenism. For instance, when the CDC merely informs patients about a policy, this is a form of tokenism because no real opportunity to influence the policy is provided. Patients are treated as empty heads that need to be filled with information provided by the CDC. It’s a one-way street.
And, if the information provided by the CDC is biased, it may actually be a form of manipulation. For example, when the CDC says that patient deaths have occurred in the treatment of Lyme disease, but neglects to mention that these are quite rare, it is a form of manipulation. Patients are not being told the facts—they are being given a dose of opinion intended to influence their behavior. Even when patients are given voice—an opportunity to say what matters to them—if they do not have an opportunity to affect real change, their participation is illusory. It can become a game of “tell me what you think, but don’t expect me to take it into account when I make decisions.”
To be sure, communication is important and essential to change, but it is not sufficient to create meaningful participation for patients. Other forms of tokenism include consulting with (but not necessarily listening to) patients or placating patients by putting them on a committee that has no power. One concern patients raise about the current overtures by the CDC is whether they mark a move toward partnership—or, as some patients believe, are no more than a premarketing move to placate patients before a new vaccine hits the market. The CDC is not helping matters when it says engagement is necessary for “prevention.” What about all of the sick patients? Do they not even make the agenda?
Patients were pleased that the CDC shared results of some studies supporting the increase in Lyme cases to 300,000, but in a true partnership, patients would have known those studies were being conducted in advance. Even more—we would have had a hand in how the studies were conducted and what questions were asked. For participation to be meaningful, patients must have an opportunity to influence decision-making—to make a difference. Recently, patients have been talking with the CDC—let’s see if it makes a difference. Otherwise, communication without the ability to influence is a form of placation or tokenism.

.
.
LYME POLICY WONK blog is written by Lorraine Johnson, JD, MBA, who is the Chief Executive Officer of LymeDisease.org, formerly CALDA. Contact her at lbjohnson@lymedisease.org.






Dear Lorriane:
Thank you for your ongoing publication of thoughtful, educated and insightful articles. As a former lawyer who is still struggling to recover from Lyme, I admire your turning your considerable talents to benefit those who struggle with the disease you have overcome. I hope one day to do the same.
In response to your article, I suppose only time will tell whether the CDC’s release is tokenism or genuine engagement. I am included to believe the former. The CDC has not made any effort to revisit the very flawed guidelines yet (so flawed that an increasing number of doctors don’t even abide by them — making me wonder to what purpose those brave, early LLMDs were persecuted). Its study seems quite haphazard and inadequate (1. counting by looking at insured cases, when insurance uses the CDC’s own two-tier testing and connected IDSA guidelines to deny payment, is bizarre. 2. Counting by looking at reported cases, when the criteria requirements are scientifically unsupported, wildly difficult to meet, inaccurate, and onerous, is equally ludicrous). The reported numbers, I believe, still vastly under-count the number of true cases. Given that Alan MacDonald could not publish a peer-reviewed study showing the connection of Alzheimer’s with Lyme, and given the Embers study’s publication was mysteriously delayed for many years while Steere’s very scientifically flawed study became, de facto, the medical standard, I find it hard to put aside all cynicism and distrust and think the CDC is simply “coming clean.” The only thing that might cause that to happen is a possible reckoning based on the FOIA docs that Kris Newby finally obtained. But until the CDC takes down its ludicrous two-tier testing criteria, validates the culture test (never heard of a false positive culture test, but apparently some IDSA docs still cling to this argument) and engages actual Lyme practitioners without conflicts of interest in a speedy review and revision of the treatment guidelines, I will continue to believe that there is a hidden agenda.
Being in this twilight world of Lyme, it’s easy to become paranoid and to believe in conspiracies, especially when one is proven right as in the case of the IDSA/CDC collusion.
Thanks for your continued vigilance.
here’s what I think for what it’s worth. I think that the CDC has just softened their stance. nice… right up until you take into consideration why. it was calculated to placate the lymies into shutting up! they severly miscalculated! LYMIES are tired, hurt, losing everything and/or their children, angry & dying!!! like me they are not going down without a fight anymore!!! I think enough has been said by LYMIES to make that point to the CDC the IDSA and now they are running scared and trying another way to cover their tracks. this time they are talking as if they really want our input. maybe they are scared enough to really mean this but you teach people how to treat you. we have taught the CDC & ISLA to treat us like dirt. they have taught us how to bow and scrape for any scraps they dish out. you tell me..what’s the chances that they will change the way they do things now without us re educating them to the new reality that we are all mad as hell and not taking it anymore!!! yeah.. i thought you might see it my way!!!!
There is no question in my mind about the level of patient involvement. We are at the no power level, and being manipulated every time the CDC pretends to consult us, sends Dr. Beard to talk to one of our groups, or on the phone to activists. This has been going on for years. And you could say the same thing about NIH. Take that Klempner clinical study which was supposed to be the first in a series. Instead it used an inadequate protocol and then blasted the result out to the media, and refused to continue to study the disease in its late stage, and is undoubtedly part or all of the reason why the Embers study took so long to get published.
This is all intentional, folks. They do not actually give a flying damn about sick people.
My statements above should not be construed to mean that we should just ignore the CDC and NIH and go our own way. We need to continue to hold their feet to the fire, make them understand the harm their stance has done to individual patients and to public health as a whole.