












MEDICAL DETECTIVE: 2-week pulses of antibiotics for chronic bartonellosis

This article was originally posted on Dr. Richard Horowitz’s Medical Detective Substack. It is the final installment of a 5-part series on Bartonella. You can find more helpful content by subscribing here.
By Dr. Richard Horowitz
Bravo! You’ve made it to Part 5, the final Medical Detective blog on diagnosing and treating chronic Bartonella infections.
As you read in the previous four installments, Bartonella is often found in my chronic Lyme patients, at least 80% of the time, right behind active Babesia infections. (Watch for unexplained fevers, day/night sweats, chills, flushing, “air hunger,” and an unexplained cough if you have ongoing Babesia. See my previous 3-part Babesia series for more information. Part 1, 2, 3.)
Many of the symptoms of chronic bartonellosis overlap chronic Lyme disease. Check Bartonella, Part 2 for details.
So if you have ongoing symptoms after double dose dapsone combination therapy (DDDCT) followed by a 4-day pulse of high dose dapsone combination therapy (HDDCT), which is effective in many cases of chronic Lyme disease, active Bartonella is one of the most common reasons why you may still be ill, apart from multiple MSIDS variables increasing inflammation with downstream effects.
Differential Diagnostic Possibilities Might Explain Why You Have Resistant Symptoms Even After DDDCT Therapy
Double dose dapsone combination therapy (DDDCT) followed by a 4-day high dose dapsone combination (HDDCT) pulse is not enough to clear a Bartonella infection, although it can be very helpful in improving symptoms, just not giving you a full remission. If you still have resistant symptoms, the most common reasons why you’re still ill are:
- Active Bartonella: this is often proven by a positive Bartonella FISH test (IgeneX, T Labs) but also elevated VEGF (vascular endothelial growth factor) levels done through a local lab. An elevated VEGF can however also be seen in long COVID and in diseases causing vascular inflammation. (Look for Galaxy laboratory in your state, as they are also an excellent choice for testing with their ddPCR.)
- Active Babesia: apart from the symptoms discussed above, a positive Babesia FISH test (IgeneX, T Labs) will help to confirm the diagnosis.
- Mold toxicity: mycotoxins are often present in those with resistant Bartonella infections, and mold can cause immune suppression, as can Lyme and long COVID. A Real Times Laboratory mycotoxin test can confirm exposure (my first choice). There are other ways of confirming exposure to mold (Great Plains Lab, Vibrant Lab) via antibody testing. A Stachybotrys titer may also be positive through local laboratories implying exposure. I’ll discuss mold toxicity in upcoming Substacks.
- Long COVID: I have patients get a 14-cytokine panel through Radiance Diagnostics and look for classical markers of Long COVID. You can order the test online: covidlonghaulers.com. Long COVID can interfere with the success of DDDCT and HDDCT in part because of spike proteins causing ongoing monocyte activation with inflammation (all 16 MSIDS factors have been associated with Long COVID). Stay tuned for future Substacks discussing potential treatments for Long COVID.
- Ongoing MSIDS Abnormalities: Mast cell activation syndrome (MCAS), whether from leaky gut and Candida (with multiple food sensitivities), or due to or Lyme/Bartonella/mold, is often present in those with chronic resistant symptoms. A full MSIDS review should be done in those with ongoing symptoms post DDDCT and HDDCT to evaluate where the source(s) of inflammation are coming from. This chart shows you the multiple MSIDS factors found in my chronically ill patients:
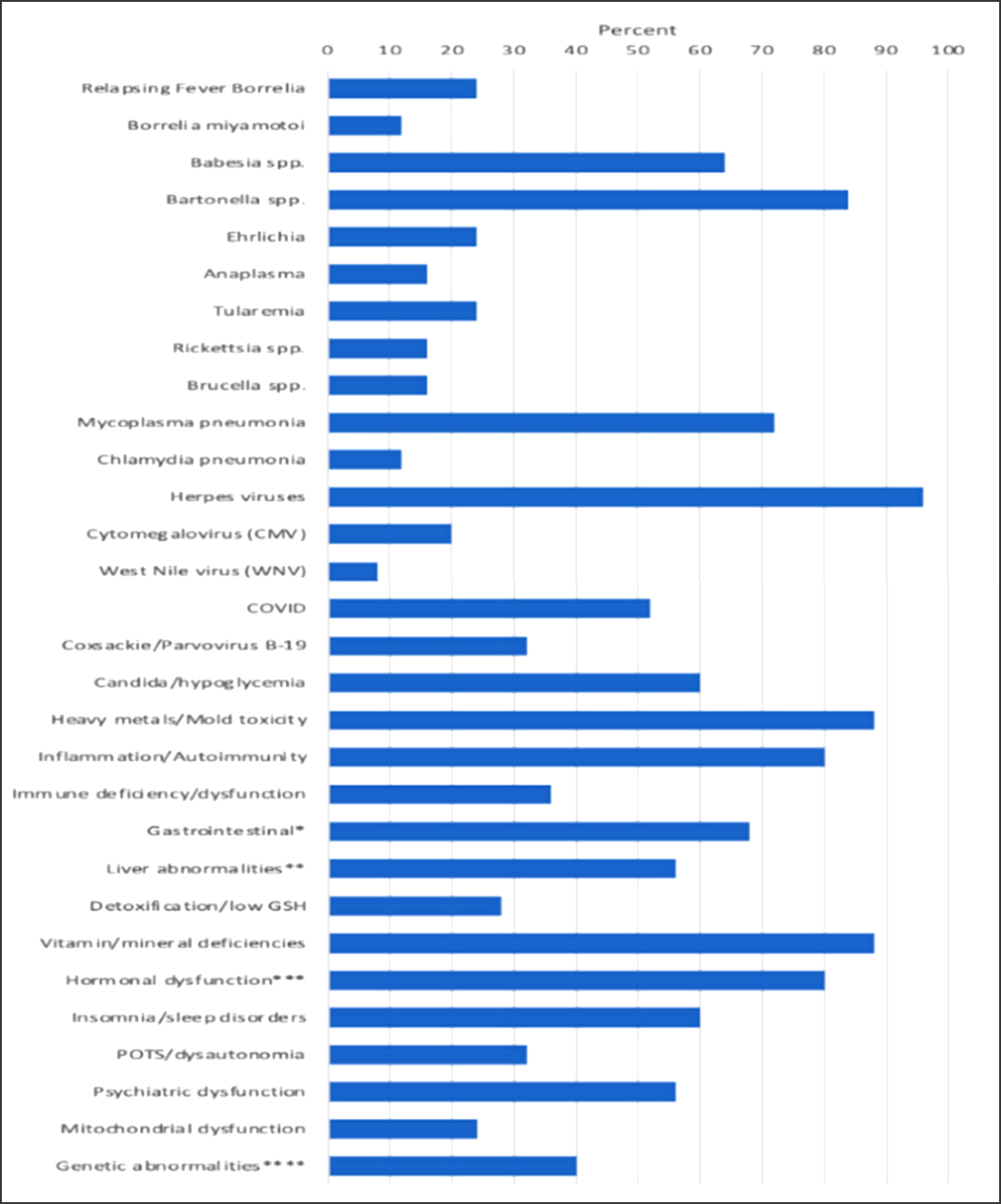
Horowitz, R.I.; Fallon, J.; Freeman, P.R. Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections. Microorganisms 2023, 11, 2301. https://doi.org/10.3390/microorganisms11092301
Once you have ruled out all overlapping sources of inflammation and downstream effects, and properly treated them, and have identified chronic Bartonella as one of the primary reasons why you are sick, the 14-day protocol listed below (also found in the above Microorganisms paper) will be helpful in getting you better when you suffer with chronic Bartonella.
THE 14-DAY HVHAC DDCT PROTOCOL, USING PYRAZINAMIDE (PZA)
This protocol is usually done after the completion of DDDCT and a 6-day pulse of HDDCT. Usually a minimum of four pulses, approximately 6-8 weeks apart is needed to adequately lower the load of Bartonella for patients to see significant improvement and remain in remission.
Those with significant amounts of mold and other MSIDS factors affecting immunity may need more pulses. In between pulses, I’ll continue to address other MSIDS variables, such as a mold/heavy metal detoxing or mitochondrial dysfunction, etc.
I prefer to use Pyrazinamide (PZA) in this protocol, as it is a mycobacterium “persister” drug that shortens the course of antibiotic therapy in TB; a 2016 publication we did showed it helpful. Much larger controlled studies will be needed, however, to confirm the importance of PZA in this protocol. Approximately 5% of patients get a rash with PZA, requiring it to be stopped, but usually the rash resolves within 48 hours with antihistamines. This protocol can be done without PZA if needed.
Weeks 1 and 2
Medications Week 1
*Please check with your healthcare provider regarding any medicine that you are taking (send over a complete list of medications and supplements) if you are unsure if it can interact with methylene blue or any other medication used during this protocol, including but not limited to rifampin, cimetidine, macrolides, etc.
*All psychiatric medicines (except for benzodiazepines) should generally be avoided while on methylene blue to avoid the possibility of serotonin syndrome.
*It is advisable to slowly increase and add antibiotics every few days during the first week of the protocol to ensure GI tolerance.
For example, on Monday, and for every day this week:
*Plaquenil (hydroxychloroquine) 200 mg once per day
*Doxycycline 100 mg twice per day with meals or minocycline 50-100 mg twice per day if there is GI intolerance to doxycycline
*Cimetidine 400 mg twice per day with meals
*Nystatin 500,00 units, two twice per day (see doses below along with biofilm agents and supplements, probiotics, etc.)
*Methylene blue 50 mg twice per day
On Tuesday continue the same protocol from Monday.
On Wednesday add:
*Rifampin (Wednesday), 300 mg twice per day
*Methylene blue is now increased to 100 mg twice per day
On Thursday add:
*Pyrazinamide. The dose is based on body weight. For example, 40-55 kg is 1000 mg once per day; 56-75 kg is 1500 mg once per day (3 tabs, 500 mg each, once per day), or if you weigh between 76-90 kg, the dose is 2000 mg once per day
*Continue Methylene blue 100 mg twice per day
On Friday add:
*Azithromycin (Zithromax) 250 mg twice per day
*Increase Methylene blue to 200 mg twice per day (400 mg by day 5, 6-7).
On Saturday and Sunday, you will continue the above medication at the same doses.
At the end of Week 1, you will therefore be on Plaquenil, doxycycline (or low dose minocycline), cimetidine, rifampin, Zithromax, PZA, Nystatin, and methylene blue.
*All antibiotics should be taken with a full stomach after breakfast and dinner.
*Tetracyclines (doxycycline, minocycline): Take with a full stomach and 8 ounces of water, sitting up for one hour post ingestion to avoid reflux esophagitis. Do not mix dairy and minerals within one hour of use. Avoid more than several minutes of direct sun as tetracyclines can cause a sunburn; use a 65 SPF sunscreen on all exposed areas (hands, face, etc.) even while driving.
*For those needing phenazopyridine (Pyridium) to decrease urinary tract discomfort while on high dose methylene blue–which can cause urinary burning in at least 50% of patients–it can be prescribed at a dose of 200 mg three times per day as needed during the protocol. Tell your healthcare provider if you have any urinary discomfort requiring this medication.
*You may need Zofran (ondansetron) for nausea while on high dose dapsone, week 2. This is not an uncommon side effect when the dose of dapsone is raised to 200 mg twice a day. The use of Zofran requires having a normal EKG and QT interval. Make sure that your HCP has a baseline copy of your EKG. It is a good idea while on Plaquenil and Zithromax to take a dose of Zofran and then go for a repeat EKG to ensure that the QT interval remains within normal limits.
*Use Zyrtec (cetirizine) 10 mg once per day with famotidine 10 mg up to 40 mg twice per day as needed for any GI upset/mast cell symptoms. Cytotec (misoprostol) 200 mcg twice per day can be used also twice a day for upper GI support, along with extra Pepcid (famotidine) which can go up to a dose of 40 mg twice per day.
*Two supplements to consider if there is still any G.I. upset: Gastromend (Designs for Health), 2 capsules twice a day away from antibiotics and Glutaloemine (Xymogen) one scoop twice a day.
Medications Week 2
Stay on the same protocol as Week 1, then do the following:
*Add dapsone 100 mg, 2 twice per day, for 6 days in a row starting Monday of week 2. This will be added to all medication taken at the end of week one.
*Double the rifampin dose to 600 mg twice per day (300 mg, two twice per day) starting Monday
*Add leucovorin 25 mg, four twice per day, with Xaquil XR (Xymogen, l-methylfolate) four twice per day (to help reduce dapsone induced anemia) starting on Monday.
*Increase methylene blue dose to 300 mg twice per day, the final dosage, starting Monday when high dose dapsone is added. Continue at this dose for 6 days.
*For those needing Pyridium (phenazopyridine) to decrease urinary tract discomfort, it can be prescribed at a dose of 200 mg three times per day while on methylene blue.
*Get a CBC, CMP Week 2 (around day 12) with a methemoglobin level.
Pulsed Antibiotic Protocol Medication and Nutritional Supplementation Diet
*Keep a home electronic blood pressure cuff, especially if you have high blood pressure, and intermittently check your blood pressure while taking MB.
*Avoid aged cheese, liver, avocados, beer, wine, overripe fruit, raisins, sauerkraut, sour cream, soy sauce, yeast extracts, etc. since a low histamine diet will help protect against any increases in blood pressure while on higher dose methylene blue (MB).
*Stay on a low carbohydrate diet and avoid simple carbohydrates to avoid promoting yeast/candida overgrowth.
*Tell your HCP if you develop any loose stools or diarrhea during the protocol since this may require stopping your antibiotics. If you are a woman, you also need to ensure that you are not pregnant, and taking proper precautions before using this regimen (rifampin affects drug levels of hormones, including the BCP)
4 biofilm agents are taken during the entire 2-week protocol
*Take cinnamon/clove/oregano oil one twice per day
*Biocidin 2 sprays twice per day
*Stevia 15 drops twice per day
*(Peppermint oil capsules one twice per day (peppermint oil capsules and methylene blue comes from Infuserve in Florida).
Support Supplements
NAC 600 mg twice a day (Xymogen)
Glutathione, a minimum of 1000 mg twice per day (Orthomolecular) first week, increase to 2000 mg 2-3 time per day week two on dapsone. Liposomal formulations of glutathione (Essential Pro, or Researched Nutritional Trifortify liposomal GSH) are also good options.
Alamax (ALA) 600 mg one twice a day (Xymogen). Watch for any hypoglycemic events (blood sugar swings) on higher dose ALA. This is a rare side effect. A strict hypoglycemic diet should stop this from happening.
Curcuplex one twice per day (Xymogen)
Oncoplex one twice per day (Xymogen)
Melatonin 1.5 mg at bedtime (half a 3 mg dose of melatonin, Xymogen)
BLT 30 drops three times per day and use Alka-Seltzer gold (sodium HCO3) two fizzy tablets up to twice per day as needed for severe Herxes with higher dose glutathione.
Vitamin C 1-2 grams twice per day, Vit E 300 IU, 1-2 twice per day, ENADA (NADH) 5 mg, two twice per day should also be used the week on dapsone, as the extra antioxidants are helpful in lowering methemoglobin levels with medication like cimetidine and methylene blue.
Probiotics
*Take Orthobiotic, Saccharomyces boulardii, and Theralac three times per day, first thing in the morning, in between lunch and dinner, and last thing before bed.
*Take ½ a packet of Probiomax 350 billion two times per day.
Once You Have Completed the 2-Week Protocol
*Stop all antibiotics, but continue on Nystatin, all probiotics and biofilm agents, and any other support supplements advised by your provider for at least the next month.
*Methylene blue (MB) should be tapered during the week off antibiotics and dapsone, by decreasing the dose to 200 mg twice per day for 2 days, 100 mg twice per day for 2 days, 50 mg twice per day for 1 day, and then stopping it.
Do not continue to use a higher dose of MB after 5 days once dapsone is stopped, as it can result in symptoms of serotonin syndrome. Blue hands/lips etc. can be seen with methylene blue and do not necessarily imply elevated methemoglobin levels. Check blood levels if there is any question. Pulse oximetry does not work while you are on MB.
Speak to Your Health Care Provider About a Mitochondrial Regeneration Protocol Post-Treatment
Mitochondrial support has been shown to be helpful in some patients with a chronic, fatiguing illness. You can stop the mitochondrial supplements after one-month post-therapy. The following supplements can be taken after breakfast and dinner.
*ATP 360, 3 per day (Researched Nutritionals)
*ENADA one per day
*Carnitex two twice per day (Xymogen, not for those with alpha gal allergy)
*CoQ Power twice per day (Researched Nutritionals)
*Cardio Ribose, one scoop twice per day, along with Mitoprime (Xymogen) one per day, and Mito NR (Designs for Health) two per day.
This protocol can also be found in our published article in Microorganisms, September 2023:

The above protocol has been completed by hundreds of my patients with good success. This is a quote I received from a fellow physician who took my training course and used the medical consultation model we offer at the HVHAC when this doctor was wanting to learn how to do DDDCT and HDDCT safely and effectively. He describes how this protocol has saved his patients life and reversed a 20-year medical sentence of poor health:
Subject: Thank you message
I have just seen a patient who is today symptom free after having suffered 20 years and he is only 31 years old. He attempted suicide at the age of 15 and was ultimately diagnosed with bipolar disorder. After the Dapsone protocol he is a new man. From being disabled, not able to work he is back to work and from his former 36 hours a week, he now works 48 hours a day. From being disabled he now works out 40 minutes before going to work. He never felt as good as now with energy and clarity of mind. From an absent father, he now enjoys parenting. I was just wanting to share this amazing Dapsone story with the author of it. Thank you for what you are doing for the Lyme disease community.
You can watch a second dapsone documentary during the Healing Lyme Summit 2.0 in April 2025 where I am co-host, with patients sharing their success with this protocol. The physician quoted above will be part of the new documentary.
The prior 2024 dapsone documentary highlights the success of 18 chronically ill patients who got their lives back with DDDCT and HDDCT: https://players.brightcove.net/6314452011001/PAMDt93Yi_default/index.html?videoId=6353288590112
Stay tuned for the next dapsone documentary which will be released April 2025. I will be providing links for the Summit (free to attend) on my Facebook page in early April:
https://www.facebook.com/drrichardhorowitz/
For those health care providers who wish to learn more about how to treat chronic Lyme disease and associated co-infections, there are training videos on my website and a consultation model where I can help with complex cases if needed (depending on time availability). Please contact my medical office for more information.
https://cangetbetter.com/healing-lyme-co-infections-training-course/

You now have the tools to help treat chronic Bartonella infections. As an aside, once patients have gotten through the DDDCT protocol with several HDDCT pulses, I’ve occasionally found that 13-day pulses can be done without dapsone and still provide some relief, but my general experience is that the protocol works best with dapsone.
Those with anemia or who are unable to do dapsone because they lack G6PD, may still get some benefit from pulsing antibiotics with multiple persister drugs and biofilm agents. I’ve submitted a grant for a multi-center, placebo-controlled randomized trial of DDDCT and HDDCT for the treatment of CLD and associated co-infections, so stay tuned as I work through the process to make this a reality.
In the meantime, please share this 5-part series on Bartonella with those who are chronically ill. It is the shortest, most effective treatment you can use.
Wishing you blessings of health and healing.
Dr. Richard Horowitz has treated 13,000 Lyme and tick-borne disease patients over the last 40 years and is the best-selling author of How Can I Get Better? and Why Can’t I Get Better? You can subscribe to read more of his work on Substack or join his Lyme-based newsletter for regular insights, tips, and advice.






We invite you to comment on our Facebook page.
Visit LymeDisease.org Facebook Page