













- sinus node disease, marked by alterations to the heart’s “motor” or natural pacemaker,
- atrial fibrillation, which is a disorganization of the cardiac rhythm that increases the risk of stroke,
- bundle branch blocks, or lesions in the distal cables of the heart that can interrupt electrical impulses, and
- myocarditis, pericarditis or endocarditis, which are different degrees of inflammation of the layers of the cardiac walls.
Some of these manifestations can be so severe that total cardiac dysfunction may rapidly occur, and the patient may die despite medical efforts. Sometimes a heart transplant is the only option.
Diagnosing and treating Lyme carditis
The initial symptoms of Lyme disease can be mistaken for other common infections or allergic reactions. Delayed diagnosis and delayed initiation of proper treatment can lead to serious Lyme disease presentations including Lyme carditis in all its forms.
We need ongoing education at all levels (medical and nursing schools, community, governments) to close the gap in knowledge and ensure all participants in the health-care system aware of this preventable condition.
The good news is that prompt diagnosis and appropriate antibiotic therapy leads to a much better prognosis. Lyme carditis responds very effectively to treatment, completely eliminating the cardiac manifestations, with a very favourable prognosis in both short- and long-term followup. We now know that when antibiotics are used according to guidelines, the prognosis two years after the infection reveals no residual disease in the heart.
It is important to remember that most heart conduction abnormalities caused by Lyme carditis resolve with appropriate antibiotic therapy without requiring the implantation of permanent pacemakers. As most patients presenting with Lyme carditis are young and otherwise healthy, any medical strategy that could prevent the need to implant a pacemaker for the rest of their lives is welcomed.
Confirming Lyme disease in the age of COVID-19
The current COVID-19 pandemic is posing a new challenge in the diagnosis of Lyme disease. The two conditions have a lot of overlapping symptoms, such as fever, malaise, generalized pain and lack of energy. During these times, it’s advisable to rule out COVID-19 first before embarking on any other test.
Asking focused questions about personal lifestyle may help guiding the diagnosis of Lyme disease. Some key questions include:
- Any outdoor activities in areas already identified as having high prevalence of ticks?
- Any recollection of tick bites or removal of ticks from the body?
- Any skin rashes? (Remember that the classic bull’s-eye rash is only present in about 40 per cent of cases and non-specific rashes can also occur),
- Do you live in an endemic region for Lyme disease? If you’re not sure, you can check public health websites. Knowing if one lives in an endemic region for Lyme disease is essential, as these recommendations should be encouraged in all emergency departments and family doctors’ offices in areas of high prevalence.
Skin examinations and ECGs
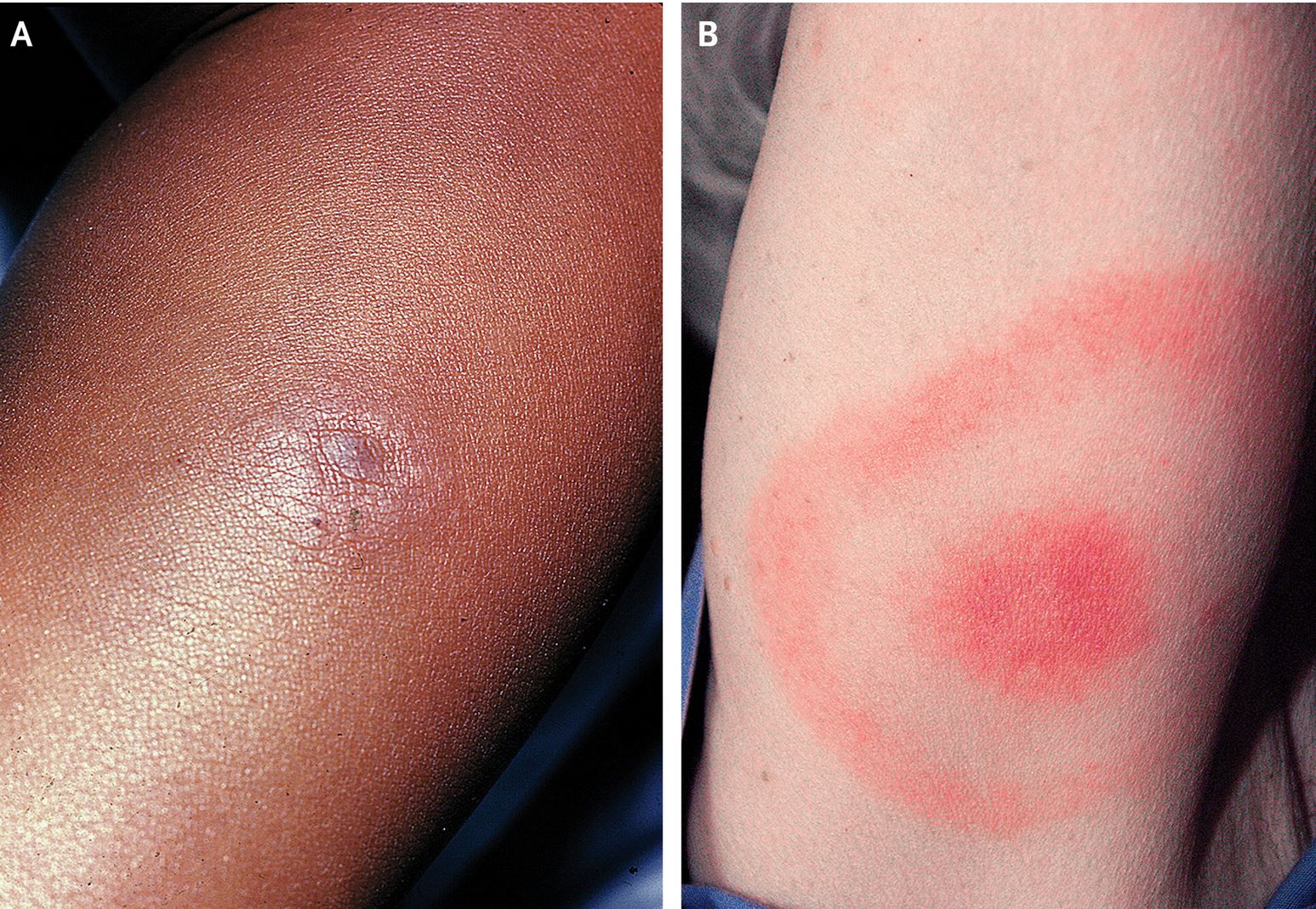
A bull’s-eye-shaped rash is a characteristic symptom of Lyme disease, but it isn’t present in all patients. Some have a less defined rash.
Thorough dermatological examination can clarify difficult cases. This happened in my clinic recently, when a nurse practitioner decided to run a full skin examination and discovered typical bull’s-eye rashes on the patient’s back.
Once the diagnosis is suspected, cardiovascular symptoms such as dizziness, palpitations, fainting or near fainting, chest pain and shortness of breath should be investigated. If the patient reports any of these symptoms, along with any other factors suggesting Lyme disease, a 12-lead ECG (the simple and inexpensive electrocardiogram) should be performed.
Quite recently, a team from the United States did 12-lead ECG to a large series of pediatric patients presenting to the emergency department with high-suspicion of Lyme disease, and discovered that nearly 30 per cent of them had some conduction disturbance. Any evidence of electrical disturbance should prompt admission in hospital for a course of intravenous antibiotics while waiting the results of serological tests.
Suspicious Index in Lyme Carditis
From the other perspective, any patient presenting with unexpected high-degree atrioventricular block (full electrical shut down of the electrical system of the heart), the way to test for Lyme carditis is by running a risk score called SILC (Suspicious Index in Lyme Carditis), which was developed at Queen’s University and is now used worldwide.
SILC score is based on the risk factor acronym COSTAR (Constitutional symptoms, Outdoor activities/endemic region, Sex male, Tick bite, Age < 50, Rash), which may help in determining the likelihood of early Lyme carditis.
We need to keep teaching and learning about Lyme carditis. In addition to ongoing education, curricula in medical and nursing schools should be updated immediately to be sure that all new health-care providers are trained in the rapid recognition of this condition. When to order serological tests, how to check for cardiovascular symptoms and the value of the 12-lead ECG are all important steps in the management of Lyme carditis.
The effort to eradicate Lyme disease should involve physicians and nurses, patients and families, rigorous science and political decisions for sound policy implementation.![]()
Dr. Adrian Baranchuk is a cardiologist and Professor of Medicine, Queen’s University, Ontario Canada. This article is republished from The Conversation under a Creative Commons license. Read the original article.






We invite you to comment on our Facebook page.
Visit LymeDisease.org Facebook Page