












MEDICAL DETECTIVE: Effective treatments for Bartonella infections

This article was originally posted on Dr. Richard Horowitz’s Medical Detective Substack. It is Part 3 of a 5-part series. You can find more helpful content by subscribing here.
By Dr. Richard Horowitz
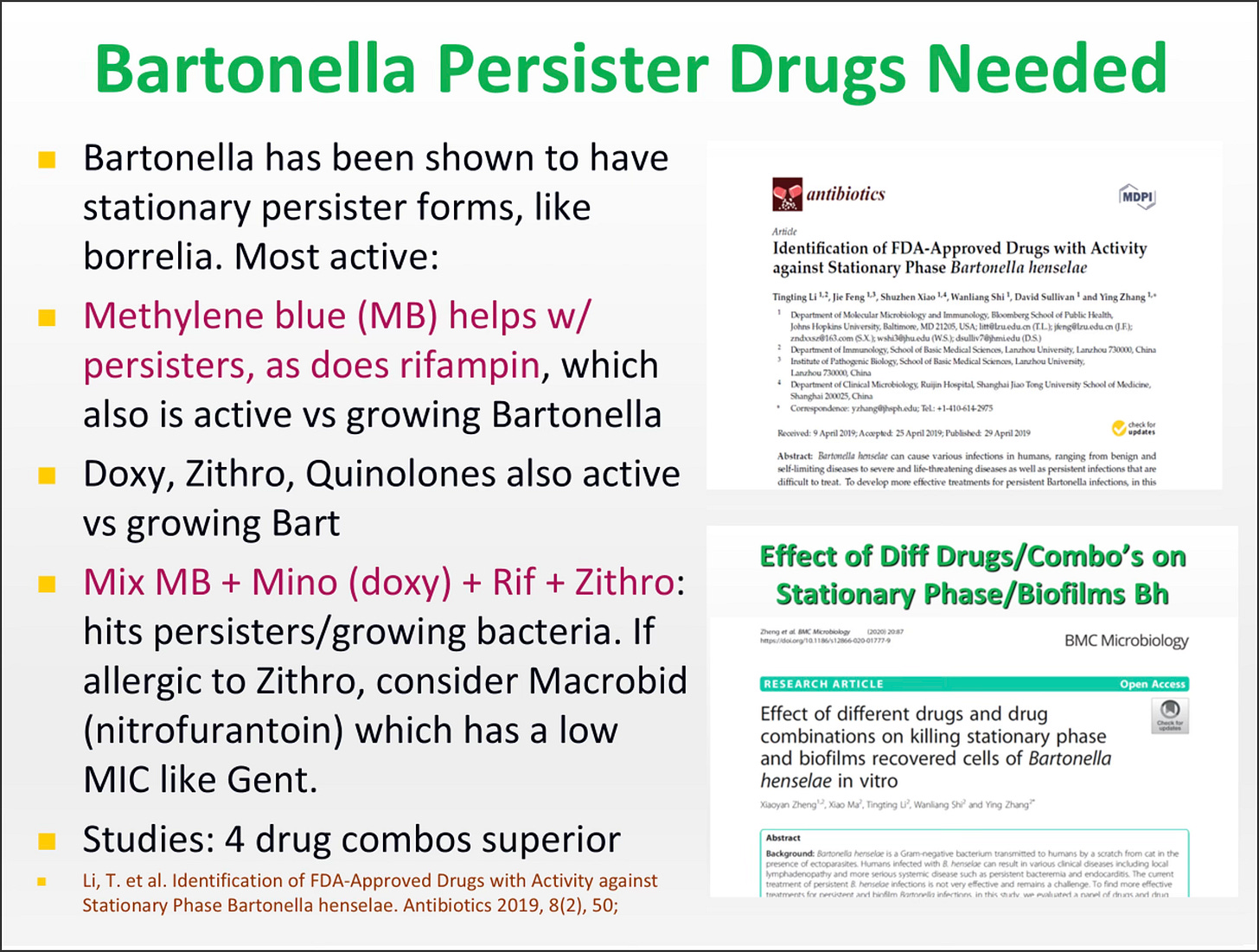
Bartonella is an intracellular biofilm/persister bacteria, like Borrelia burgdorferi, the bacterial agent of Lyme disease.
For years, many doctors were using single drug therapies for Cat Scratch Disease (CSD)–a form of Bartonella infection–even in the chronic persistent phases of the infection (some may still).
This was before we understood the complexity of how this bacteria persists.
Years ago, however, I did recognize that at least two intracellular antibiotics were more effective than one for difficult-to-treat intracellular infections. So for many years I treated Bartonella with doxycycline/rifampin or Zithromax/rifampin. Although they helped to knock down symptoms, Bartonella would invariably return after antibiotics were stopped. Persisters persist!
Figuring out how to treat Bartonella and chronic Lyme
If someone would’ve told me decades ago that I would have found a durable solution and potential “cure” for a worldwide epidemic of chronic Lyme disease, I would’ve laughed and told them that they are drinking too much of the Kool-Aid.
It is of course a dream of any physician to make a difference in the world and find a solution for millions of people who are chronically ill. Yet when University-based researchers discovered that Borrelia was a biofilm/persister bacteria, I realized that I’d had experience treating “persister” bacteria when I was at Elmhurst Hospital in Queens during the HIV epidemic.
Many of those patients who were immunosuppressed had come in with MAI (Mycobacterium Avium Intracellulare) and Mycobacterium tuberculosis (TB). I had experience using medications like INH, rifampin, and pyrazinamide, and felt comfortable using these persister drugs. So I reviewed studies about the Mycobacterium drugs used for TB and leprosy in the medical literature. The moment I came upon dapsone, I realized that it was going to be a winner.
Dapsone fit all the criteria and checked all the boxes. It was a persister medication used in combination with rifampin to treat leprosy, and one year of combination therapy resulted in a cure for many patients.
It had excellent penetration into the Central Nervous System (CNS) and might enable me to avoid using IV medications like Rocephin. It treated autoimmune diseases like Behcet’s syndrome, and we saw autoimmune phenomenon all the time in our chronic Lyme disease patients.
It lowered inflammation, the primary reason why most people stay ill with chronic infections and toxins. And it had antimalarial properties. This would potentially allow me to treat Babesia at the same time, another chronic infection making my patients ill. (See prior Medical Detective Substacks on the topic.) With the help of Dr. Eva Sapi and her students from the University of New Haven, we proved that dapsone is also effective for the biofilm/persister forms of Borrelia burgdorferi.
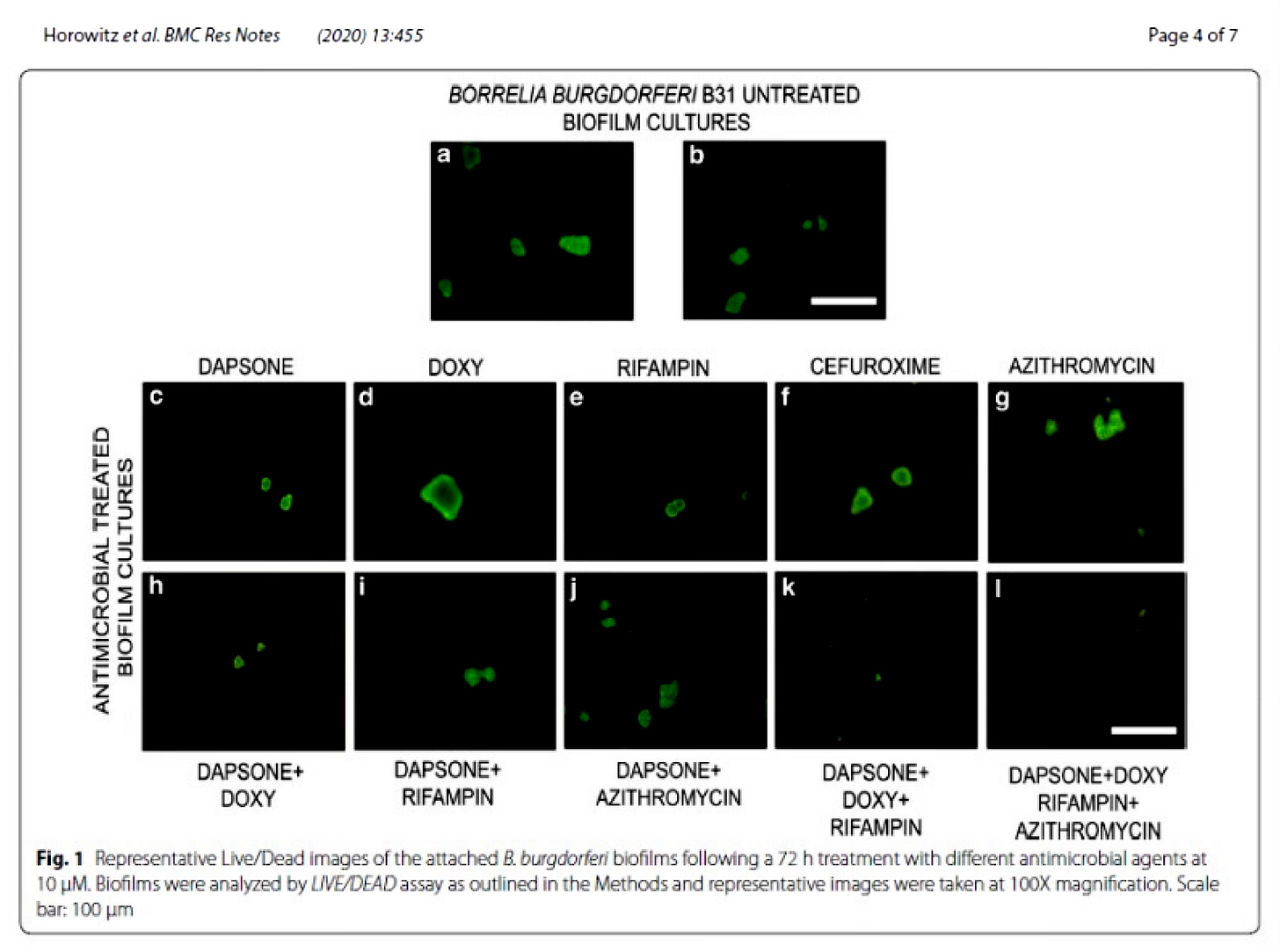
[From: Horowitz, R.I., Murali, K., Gaur, G. et al. Effect of dapsone alone and in combination with intracellular antibiotics against the biofilm form of B. burgdorferi. BMC Res Notes 13, 455 (2020). https://doi.org/10.1186/s13104-020-05298-6]
Combination therapy
You can see from the above images that dapsone alone was effective in treating the biofilm forms of Borrelia (better than doxycycline), and the more medicine we used in combination therapy, the better it worked (4 drugs were better than 3, which were better than 2, which were better than solo drug therapy).
Dr. Phyllis Freeman and I published the first article on dapsone combination therapy for the treatment of chronic Lyme disease back in 2016, in 100 sick patients: Horowitz RI, Freeman PR (2016) The Use of Dapsone as a Novel “Persister” Drug in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome. J Clin Exp Dermatol Res 7: 345. doi:10.4172/2155-9554.1000345.
It was exciting, because even low doses of the medication alone and in combination had an effect on most of major Lyme symptoms making my patients ill.
Year after year, I continued to publish on different doses of dapsone in combination with other medications, trying to improve the efficacy rate, until I got to the point where I found that DDDCT (double dose dapsone combination therapy, 100 mg twice a day) got approximately 50% of the patients with chronic Lyme disease into long-term remission for one year or longer with only 8 weeks of oral, generic antibiotics, using dapsone in combination with a tetracycline and rifampin, and occasionally azithromycin.
The patients who didn’t improve? They had Babesia and/or Bartonella! Babesia interfered with the efficacy of the double dose dapsone protocol, as it did in our first publication listed above, as did Bartonella.
You can read about it in this article: Horowitz, R.I.; Freeman, P.R. Efficacy of Double-Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post-Treatment Lyme Disease Syndrome (PTLDS) and Associated Co-infections: A Report of Three Cases and Retrospective Chart Review. Antibiotics 2020, 9, 725. https://doi.org/10.3390/antibiotics9110725
The current treatment protocol for chronic bartonellosis and chronic Lyme disease at the Hudson Valley Healing Arts Center
The initial protocol for chronic Lyme disease at the HVHAC is 8 weeks of double-dose dapsone combination therapy (DDDCT) followed by 4 days of high dose dapsone combination therapy (HDDCT).
In many cases, this may be enough to knock down the load of the persisters and lead to significant clinical improvement (if all MSIDS variables like mold, Covid longhauler syndrome, other co-infections, etc. are not active and present).
If you have Bartonella as well as chronic borreliosis, 8 weeks of DDDCT and a minimum of four, 6-day pulses of HDDCT, at least 6-8 weeks apart, is necessary to lower the bacterial load of Bartonella to sufficiently to put most patients in remission. Those with mold toxicity, Covid longhauler syndrome and other MSIDS factors may require more pulsing for Bartonella.
I am going to list the protocol below in the link, and be aware, it is a lot of pills to take every day and requires a motivated doctor and patient to get through this.
This protocol has a lot of moving parts, but it was carefully designed and tweaked over 8 years, to minimize side effects and maximize efficacy. We don’t yet have one giant pill where all of these medications and supplements are put into a single capsule! See the David Skidmore cartoon below, that he sent me years ago:
[Cartoon by David Skidmore, used with permission.]
Although this regimen is extremely beneficial, it is crucial for you and your doctor to be aware of the potential side effects and how to address them. These are discussed in detail in our published paper: https://doi.org/10.3390/microorganisms11092301.)
Speak to your doctor about this protocol if you have tried other regimens and are still ill. It is a simplified version of the protocol we published in Microorganisms in September 2023: Horowitz, R.I.; Fallon, J.; Freeman, P.R. Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections. Microorganisms 2023, 11, 2301. https://doi.org/10.3390/microorganisms11092301
I will discuss the details of DDDCT and HDDCT in Bartonella Parts 4 and 5, but before starting this protocol, you must do the following to ensure safety
- Have your blood checked. You must be G-6-P-D positive (glucose 6 phosphate dehydrogenase deficiency would lead to increased hemolysis and anemia and higher levels of methemoglobin, a side effect of dapsone); and you must have all underlying causes of anemia addressed (B12, folate, Fe deficiency, etc.) with a minimum hemoglobin of 13.5 grams or higher. (The higher the hemoglobin, the easier it is to do the protocol, otherwise it may need to be started and stopped to let blood counts come up). Your vitamin and mineral levels (especially iron) should be normal.
- Have a normal EKG (some of the medication can affect the QT interval, potentially increasing arrythmias, although this is a very rare side effect).
- Have normal GI function (no diarrhea) and be clinically able to handle Herxheimer reactions. Herxheimer reactions are when the bacteria are being killed off, and can lead to not only temporary increases in fatigue, pain, headaches, cognitive issues, palpitations, and insomnia, but also, especially in the case of Bartonella, mood swings with increased depression, anxiety, anger outbursts, etc. For those with a history of Bartonella rage, or severe psychological issues, we suggest close monitoring by the treating physician, and consultation with a psychiatrist may be advisable.
- Provide a list of all medications and supplements for your doctor to review, as medication interactions can occur (i.e., rifampin, cimetidine, clarithromycin, and methylene blue can potentially affect drug levels). All psychiatric medications (SSRIs, buproprion, narcotics, stimulants, etc.) that could interact with methylene blue (MB) should be tapered and stopped before starting methylene blue to avoid serotonin syndrome.
- Make a list of all these foods and drinks to avoid: aged cheese, liver, avocados, beer, wine, overripe fruit, raisins, sauerkraut, sour cream, soy sauce, and yeast extracts. A low histamine diet will help protect against any increases in blood pressure while on higher dose methylene blue (one of the side effects, which is rare, but controlled with a low histamine diet).
- Stay on a strict low carbohydrate diet and avoid simple carbohydrates/sugars to avoid promoting yeast/candida overgrowth in the GI tract.
- Take tetracyclines with a full stomach and an 8-ounce glass of water, sitting up for one-hour post-ingestion to avoid reflux esophagitis.
- Do not mix dairy and minerals within one hour of use of tetracyclines, as it can interfere with absorption.
- Avoid more than several minutes of direct sun on tetracyclines (doxycycline, minocycline) since they can potentially cause a sunburn. Use an SPF sunscreen of at least 65 on all exposed areas (hands, face, etc.), even when driving.
About Methylene Blue (MB) and Its Potential Side Effects
Methylene blue is an antioxidant salt with medicinal properties, but it can cause serotonin syndrome, where your brain’s serotonin receptors can be overstimulated and lead to the side effects below. They can be avoided by slowly increasing the dose of MB during the dapsone protocol, over several weeks (see below), and making sure you are off any medication that could increase side effects, especially psychiatric medications. If any of these symptoms appear, methylene blue should be tapered quickly and dapsone stopped:
- Mental status changes: Anxiety, restlessness, confusion, disorientation, delirium, agitation, or startling easily
- Autonomic manifestations: Sweating, tachycardia, hyperthermia, hypertension, vomiting, or diarrhea
- Neuromuscular hyperactivity: Tremor, myoclonus, hyperreflexia, or bilateral Babinski sign
- Other symptoms: Dilated pupils, loss of muscle coordination, headache, shivering, or goose bumps.
About Methemoglobinemia
One of the other side effects of dapsone is elevated methemoglobin levels. This happens when there is too much oxidative stress in the body, affecting oxygen-carrying capacity in the blood. We like to have patients off any medication that can increase methemoglobin levels. That includes drugs like Tylenol and certain anesthetics.
The higher doses of MB used in this protocol, along with the other supplements in the doses below generally do an excellent job of keeping down methemoglobin levels. The average level of methemoglobin on high dose dapsone (HDDCT) the last week of the protocol is around 5-6% for 2/3 of those taking it, which can result in some increased fatigue, headaches, shortness of breath, etc., but this level is well tolerated by most individuals.
It is rare to ever see a methemoglobin level above 20% (50% or higher is dangerous). MB turns your urine/stools blue—this is normal!–and can also cause blue hands/blue lips, so the only way to know if methemoglobin levels are high is to go to the lab and check a blood level.
You CANNOT use pulse oximetry at home to measure your oxygen levels on this protocol, because MB interferes with the accuracy. You need to go to the lab and get a CBC, CMP and methemoglobin intermittently on DDDCT and HDDCT.
The protocol on when and how to do lab work on dapsone combination therapy is found in our published paper: https://doi.org/10.3390/microorganisms11092301.
Additional Information About the Dapsone Protocol Before You Start
Biofilm agents
Because both Bartonella and Lyme are biofilm bacteria, these supplements will help to open biofilms so that the antibiotics can penetrate where they need to go. They can be ordered online and also from a compounding pharmacy. Take:
- Cinnamon/clove/oregano oil twice a day (oil of oregano 1 twice a day can be used if there is intolerance to cinnamon or cloves). We use Doctor Inspired Formulations.
- Biocidin 2 sprays twice a day (work up the dose)
- Stevia 15 drops twice a day (NutraMedix)
- Peppermint oil capsules one twice a day (compounded from Infuserve in Florida).
- If you have had severe/resistant symptoms, speak to your doctor about adding on Argentyn 23, 1 teaspoon twice a day during the last month of the protocol with or without EDTA suppositories (Detoxamine) the last week of the protocol for extra biofilm support.
Probiotics
You may develop loose stools or diarrhea; if so, you might need to stop taking any antibiotics. The probiotics Orthobiotic (Orthomolecular), Saccharomyces boulardii (Orthomolecular), and Theralac (Master Supplements) will help. Take them twice a day, first thing in the morning and last thing before bed, along with half a packet of Probiomax 350 billion twice a day (Xymogen).
In most individuals, these 4 probiotics twice a day will protect the GI tract from diarrhea. In those who don’t tolerate antibiotics well, the protocol may need to be adjusted, pulsing medication.
Use Pyridium If You Have Any Urinary Burning
Tell your doctor if you have any urinary discomfort on higher doses of MB, as you can be prescribed phenazopyridine (Pyridium, 200 mg three times a day is oftentimes needed during the last weeks of the protocol) to decrease your symptoms. This doesn’t usually happen until MB doses are above 100 mg twice a day.
Checking EKG/QT Intervals
Nausea is not an uncommon side effect when the dose of dapsone is raised to 200 mg twice a day. The use of Zofran (ondansetron) requires having a normal EKG/QT interval. While on Plaquenil and Zithromax, take a dose of Zofran (all three medication can prolong the QT interval), and go for a repeat EKG to ensure that the QT interval remains within normal limits. Some patients may need Zofran 8 mg three times a day around the clock to help with nausea. It is rare for the protocol to be stopped due to nausea or vomiting the last week on HDDCT. If so, a HDDCT pulse for Bartonella may need to be done.
Lab work needed
Get labs toward the end of the third week during Month 1 of the Dapsone protocol (CBC, CMP, methemoglobin).
Get labs weekly during Month 2 of DDDCT (Double dose dapsone combination therapy) with a weekly CBC, CMP, and methemoglobin level, and also repeat these labs the last week (week 9) around day 3 or 4 of the HDDCT pulse.
Any significant lab abnormalities, including anemia with an unusual drop in blood counts (the average drop in hemoglobin is around 4 grams towards the end of DDDCT which should be expected; but can be higher, i.e., a maximum of 6 grams on HDDCT) may require holding dapsone and raising folic acid supplementation.
Keep in mind, the blood counts have ALWAYS returned to normal by weeks 6-8 after the protocol is stopped, as long as you follow the advice below on support supplements and folic acid supplementation with both Leucovorin and L-methyl folate (Xaquil XR, Xymogen).
I have seen blood counts come back up quickly once dapsone is stopped, staying on high dose folic acid, with B12 and iron, but starting with a higher hemoglobin makes this protocol easier to do, because then it does not have to be started and stopped.
Training course
I have a training course on my website, where I have trained hundreds of doctors in this protocol. It is advisable to fully understand what to expect on dapsone and how to work around side effects. Your doctor can access the training course below. It allows them to contact me (on a limited basis) to ask questions once they have completed the course.
I also have a consultation service that I offer to help doctors and patients. This is a paid service where you can have hand holding and oversight by me, but it has to be with a health care provider who understands the protocol and is willing to prescribe the medications and supplements. More information is available by contacting medical@hvhac.com.
Despite the number of pills and medication, and the complexity of the protocol, people who have been sick for decades have found relief with this 9-week oral, generic antibiotic protocol, followed by 2-week antibiotic pulses for chronic Bartonella.
I tell my patients and doctors that this regimen is like cancer chemotherapy. It is not easy to do, but well worth the long-term benefits. In those who have overlapping MSIDS variables increasing inflammation and making them sick, like mold, when they are off DDDCT and HDDCT, I then have them work on detoxing the mold or addressing other factors keeping them ill.
Support supplements
To keep down oxidative stress, support detoxification, and help reduce Herxheimer reactions, you should use several different nutraceuticals during the protocol. These include:
- NAC 600 mg twice a day
- Glutathione 4 capsules (250 mg each) twice a day
- Alamax (Xymogen, alpha lipoic acid) 600 mg, one twice a day (watch for hypoglycemia)
- Curcuplex (Xymogen) 500 mg, one twice a day,
- Sulforaphane glucosinolate (Oncoplex ES, Xymogen) 30-100 mg, one twice a day
- Vitamin C 1-2 g twice a day
- Vitamin E 300 IUs twice a day
- ENADA 5 mg twice a day
- Alka-Seltzer gold or sodium HCO3 (bicarbonate) can be used as needed for severe Herxheimer reactions, which is used with 2 grams of glutathione all at once, up to three times daily until the Herxheimer reaction resolves.
- Mycelex troches (clotrimazole) 2, 4 times per day can be used as needed if any yeast arises on the tongue. Keep down simple carbs to avoid this problem.
- You can also use up to 2000 mg of glutathione 3 times per day if there are symptoms of methemoglobinemia (blue hands, blue lips, headaches, fatigue, shortness of breath).
In Bartonella Part 4, I will explain in more detail, week by week, how to do DDDCT, and in Bartonella Part 5, I’ll discuss the 2-week HDDCT treatment and how to address MSIDS abnormalities in between pulsing antibiotics.
Dr. Richard Horowitz has treated 13,000 Lyme and tick-borne disease patients over the last 40 years and is the best-selling author of How Can I Get Better? and Why Can’t I Get Better? You can subscribe to read more of his work on Substack or join his Lyme-based newsletter for regular insights, tips, and advice.






We invite you to comment on our Facebook page.
Visit LymeDisease.org Facebook Page